 Skip to content
Skip to contentOUR PRODUCTS ARE NOT DIETARY SUPPLEMENTS OR MEDICATIONS.
OUR PRODUCTS ARE NOT DIETARY SUPPLEMENTS OR MEDICATIONS.
Product Usage: This PRODUCT IS INTENDED AS A RESEARCH CHEMICAL ONLY. This designation allows the use of research chemicals strictly for in vitro testing and laboratory experimentation only. All product information available on this website is for educational purposes only. Bodily introduction of any kind into humans or animals is strictly forbidden by law. This product should only be handled by licensed, qualified professionals. This product is not a drug, food, or cosmetic and may not be misbranded, misused or mislabeled as a drug, food or cosmetic.
RETA 20mg
$229.99
RETA 20mg
Reta is a GGG tri-agonist that targets GLP-1 and GIP receptors, akin to standard GLP-1 agonists, but also uniquely activates the glucagon receptor. This extra receptor interaction enhances glucagon production, leading to the breakdown of stored fats and glycogen, thereby increasing basal metabolism for more consistent fat loss. Its actions on GLP-1 and GIP receptors promote delayed gastric emptying and appetite control, offering a comprehensive approach to obesity research distinct from older GLP-1 agonists. Further research is required.
$229.99
Peptides will arrive in a lyophilized (powder) form for maximum stability
RETA Overview
Reta is a new entrant into the rapidly-expanding space of anti-obesity peptides. It is known as a GGG tri-agonist. This means that retatrutide works at all of the incretin receptors including GLP-1 and GIP as well as the glucagon receptor itself. Research indicates that retatrutide may be the most effective weight loss peptide yet developed, with some studies showing a rapid and sustained weight loss response as high as 24% of total body weight[1]. Reta is thought to promote weight loss by increasing energy expenditure as well as decreasing energy consumption. It does the former via action at the glucagon receptor and the latter through both central and peripheral appetite control.
RETA Structure
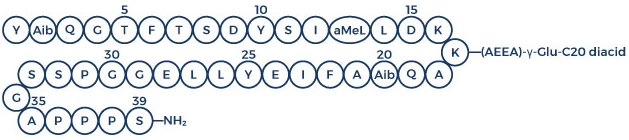
Sequence: YA1QGTFTSDYSIL2LDKK4AQA1AFIEYLLEGGPSSGAPPPS3
Molecular Formula: C223H343F3N46O70
Molecular Weight: 4731.33 g/mol
PubChem SID: 474492335
CAS Number: 2381089-83-2
Synonyms: LY-3437943, NOP2Y096GV
RETA Research
What is Reta?
Reta, as mentioned, is a GGG tri-agonist. Reta is a fatty acid acylated single peptide that combines GCGR, GIPR, and GLP-1R activities. It is based off of the GIP peptide backbone that is heavily modified. Modification of this backbone has allowed retatrutide to bind to albumin in the bloodstream. This, in turn, means that the drug remains in the blood for a prolonged period of time. This extended half-life means that retatrutide only needs to be taken once per week[2]. It wide spectrum of activity allows retatrutide to bind to several difference incretin receptors and produce specific effects as follows.
Gastric Inhibitor Peptide Receptor (GIPR): Also called the glucose-dependent insulinotropic polypeptide receptor, this receptor is found in the central nervous system as well as throughout the GI tract and body. It appears to play important roles in the central mechanisms that affect hunger and is thought to play a role in sending “fullness” signals from the GI tract to the brain.
Glucagon-like Peptide Receptor-1 (GLP-1R): Activation of this receptor leads to slowing of gastric emptying. Slowed gastric emptying sends signals to the brain to decrease food intake and can therefore help to control energy consumption. Peptides targeting this receptor were originally developed to treat type 2 diabetes, but have since been found to improve weight loss and decrease the risk of certain forms of heart disease. They are under investigation for the treatment of depression, reward system disorders (e.g., alcoholism, addiction), polycystic ovarian syndrome, and non-alcoholic fatty liver disease.
Glucagon Receptor (GCGR): The glucagon receptor is found mainly in the liver and kidney. Mutations in this receptor are associated with certain forms of type 2 diabetes. By binding to this receptor, reta increases glucagon production, which stimulates the breakdown of stored forms of energy like fat and glycogen. This leads to an increase in basal metabolism (even during sleep) that increases weight loss in general and fat loss specifically.
How Does Reta Work?
In vivo research, in humans, indicates that retatrutide activates and is a full agonist of all of the incretin receptors including GIPR, GLP-1R, and GCGR. Reta was specifically designed to be highly potent at the GIPR and GLP-1R locations. As a result, reta is one of the most potent incretins available and thus has strong effects on both gastric emptying and the central control of hunger/satiety. Research shows that the bulk of reta’s effects are driven by loss of fat mass that is probably the result of a larger and more prolonged reduction in food intake compared to similar peptides. Decreased food intake, especially as occurs early in the use of the peptide, jump starts fat oxidation. This sets the stage for prolonged weight loss by altering basal metabolism and overcoming the hormonal forces that perpetuate obesity[2].
The bulk of reta’s benefit is a result of its ability to decrease energy intake via delayed gastric emptying and increased control of hunger signals in the central nervous system. That said, the ability of the peptide to increase energy expenditure is also statistically significant and should not be discounted.
GIPR Effect: (glucose-dependent insulinotropic polypeptide receptor)
Agonism of the GIPR leads to decreased gastric acid secretion and gastrin release. Gastrin is a peptide hormone that stimulates the release hydrochloric acid and histamine in the stomach. These effects help to slow digestion and reduce transit through the GI tract. As a result, action on the GIPR can lead to increased feelings of fullness.
GLP-1R Effects: (glucagon-like peptide-1 receptor)
Agonism of the GLP-1R is well known to delay gastric emptying. Research in both rodents and humans supports this. Gastric emptying (GE) is an important determinant of the glycemic response following food intake. Research indicates that slowing GE can reduce food intake and thus impact weight loss.
Research in mice reveals that GLP-1R is the only receptor of the three to affect GE, and thus the delay of GE caused by reta is no greater than the delay caused by sema, tirz, lira, or any of the other GLP-1R agonists. Interestingly, however, is the difference in dose to achieve full effect on GE. Research shows that reta has the same efficacy as semaglutide at a dose that is more than 30 times smaller[3]. As with sema, however, the effects of reta on GE wane over time. This decrease in effect of a therapeutic over time is referred to as tachyphylaxis and may, in some cases, necessitate a drug holiday to help restore effects.
GCGR Effects: (G-protein-coupled receptor)
It wasn’t fully understood until relatively recently that glucagon plays an important role in regulating hunger and energy expenditure. Research now reveals that glucagon signals the brain from the gut via the vagal nerve. This signaling promotes feelings of fullness and is regulated by glucagon concentrations in the portal circulation of the liver. In mouse models, the administration of glucagon has resulted in a 20% weight loss[4].
Additional research has shown that glucagon can increase energy expenditure. This effect has been observed in both animal and human trials. This particular effect is not mediated through the GCGR, but rather through via FGF21. FGF21 is a protein secrete by the liver that regulated sugar intake and preferences for sweet foods, among a host of other functions. Mutations in this protein have been identified in those with a “sweet tooth” [5]. FGF21 regulates the uptake of glucose by adipocytes (fat cells). Treatment of animals with FGF21 results in increased energy expenditure, fat utilization and lipid excretion. Studies in mice show that activation of FGF21 can lead to a 20% weight reduction primarily via increased fat loss[6]. This occurs without a change in total calorie intake, indicating a change in metabolic rate. Mice given an FGF21 infusion have demonstrated higher energy expenditure both during wakefulness and during sleep. This is likely mediated through effects on mitochondrial activity.
How Effective is Reta for Weight Loss?
Research indicates that retatrutide is likely the most effect incretin-based peptide for weight loss yet developed. In a study in rodents, for instance, just 10 days of reta treatment leads to decreases in total body weight greater than those seen with sema. This occurs when the peptides are administered at the same doses. If reta is given at a lower dose that sema, then it produces similar weight loss effects but with decreased risk of side effects[3]. Thus, retatrutide may offer an alternative treatment option for those who are somewhat intolerant of the side effects of sema.
A phase 2 study in humans has showed that reta can produced significant reductions in body weight. In fact, trial participants given the highest dose of the peptide lose approximately 20 pounds in just 12 weeks[1]. In another trial, individuals treated for 26 weeks showed changes in waist circumference ranging from -2.1 cm to -10.2 cm[7]. In other words, people taking reta in this trial lost anywhere from 1 inch to ~5 inches off of their waist in just 6 months. Finally, in a trial published in the New England Journal of Medicine, weight loss from reta varied in a dose-dependent manner over the 48 weeks of the trial. Individuals given the lowest dose of the peptide lost 8.7% of their total body weight while those given the highest dose lost more than 24% of their total body weight[8]. Similar results were published in a JAMA article as well[9].
Reta and Diabetes Research
In phase 2 trials, retatrutide has produced significant reductions in glycated hemoglobin (hemoglobin A1c) levels[10]. Hemoglobin is the compound in blood that carries oxygen. Glycated hemoglobin is hemoglobin that has been chemically linked to a sugar. High levels of glycated hemoglobin are caused by chronically high levels of blood sugar and are associated with diabetes. In fact, HBA1c levels can be used to monitor long-term blood sugar control in those suffering from diabetes. Keeping these levels lower is critical not only to good blood sugar control, but to preventing the long-term effects of diabetes including cardiovascular disease, nerve damage, kidney injury, and eye problems.
Reta and Heart Health Research
It has long been known that infusing elevated doses of glucagon into those with heart failure can augment heart rate and cardiac contractility. Pharmacological administration of glucagon, typically in milligram quantities, is commonly employed in addressing acute cardiac depression resulting from overdoses of calcium channel antagonists or beta-blockers, despite limited research in this area. Interestingly, glucagon concentrations within the normal physiological range seem to have no discernible impact on heart rate or contractility[11].
The impact of reta on heart health has not been directly assessed in humans, but it has been assessed in cynomolgus monkeys. In the past, it was thought that elevated actions of glucagon were associated with diabetes. That is to say, scientists thought that lower glucagon would lead to improved outcomes in diabetes. Thus, monoclonal glucagon antibodies, glucagon receptor antagonists (peptide and non-peptide) and molecules targeting the expression of GCGR have all been tested as potential treatments. Research on these agents, however, revealed a number of major obstacles including limited efficacy, the risk of iatrogenic hypoglycemia, and other safety issues related to lack of specificity of glucagon blockade, immunogenicity and toxicity. This really should not have come as any surprise as the rise in glucagon levels in diabetes is likely a consequence of the disease and not a cause of it.
Research also indicates that incretins have beneficial effects on the cardiovascular system by decreasing blood pressure, improving left ventricular function, endothelium-dependent vasodilation, and by increasing endothelial progenitor cells. In other words, glucagon and related molecules appear to improve heart health[12]. Supporting this notion is the fact that a number of incretin agonists (e.g. sema, lira) have been associated with improvements in cardiovascular outcomes in diabetes. As a result, these peptides are now under investigation for direct use in heart disease. Reta is likely to show improved results given its more extensive effects on glucagon levels, but the exact effects will have to await more detailed clinical and benchtop trials. These findings indicate that retatrutide and similar molecules may be beneficial to regeneration in the cardiovascular as well as helping to prevent cardiovascular disease in the first place.
As mentioned, a limited, non-clinical cardiovascular study of reta in monkeys has been undertaken. This study revealed higher heart rates at all dose levels with a dose dependent effect overall. At the same time reta was increasing heart rate, it was decreasing blood pressure in the monkeys. Unfortunately, this study was limited in both duration and number of individuals under investigation. Thus, while it can offer some foundation on which to ground speculation, it cannot provide any definitive information about reta and its long-term effects on cardiovascular health.
Reta Summary
Reta is an incretin mimetic and GGG agonist. It binds to glucagon receptors, gastric inhibitory peptide receptors, and glucagon-like peptide-1 receptors. This triple activity has been associated with significant weight loss (24% of body weight at 6 months) in clinical trials. This outcome makes reta the most effective of incretin peptides to date and thus it is under intense investigation as a weight loss agent. There is some hope that reta may also have beneficial cardiovascular effects and might therefore be useful in the treatment of heart disease complicated by diabetes as well as heart disease in general.
About the Author
The above literature was researched, edited and organized by Dr. Logan, M.D. Dr. Logan holds a doctorate degree from Case Western Reserve University School of Medicine and a B.S. in molecular biology.
Scientific Journal Author
William C. Roell, PhD. received his bachelor’s degree in microbiology and biochemistry from Miami University. He obtained his doctorate in Cellular and Integrative Physiology from Indiana University School of Medicine doing work in cellular therapy and studying metabolic changes associated with adipocyte maturation. Joining Lilly in 2000, William worked with multiple drug discovery groups providing innovative approaches to translate therapeutic concepts from bench to bedside. More recently, he has supported efforts in diabetes biomarker discovery and target identification/advancement, impacting discovery and development efforts across Lilly’s Diabetes and Complications portfolio. William and his lab currently are active in drug discovery with a focus on diabetes and obesity. He has a particular interest in mechanisms by which incretin receptor modulation contributes to the profound benefits observed clinically with existing and emerging therapeutics.
Dr. William C. Roell is being referenced as one of the leading scientists involved in the research and development of Retatrutide. In no way is this doctor/scientist endorsing or advocating the purchase, sale, or use of this product for any reason. There is no affiliation or relationship, implied or otherwise, between Peptide Sciences and this doctor. The purpose of citing the doctor is to acknowledge, recognize, and credit the exhaustive research and development efforts conducted by the scientists studying this peptide. Dr. William C. Roell is listed in [1] and [2] under the referenced citations.
Reference Citations
William C. Roell, PhD. received his bachelor’s degree in microbiology and biochemistry from Miami University. He obtained his doctorate in Cellular and Integrative Physiology from Indiana University School of Medicine doing work in cellular therapy and studying metabolic changes associated with adipocyte maturation. Joining Lilly in 2000, William worked with multiple drug discovery groups providing innovative approaches to translate therapeutic concepts from bench to bedside. More recently, he has supported efforts in diabetes biomarker discovery and target identification/advancement, impacting discovery and development efforts across Lilly’s Diabetes and Complications portfolio. William and his lab currently are active in drug discovery with a focus on diabetes and obesity. He has a particular interest in mechanisms by which incretin receptor modulation contributes to the profound benefits observed clinically with existing and emerging therapeutics.
Dr. William C. Roell is being referenced as one of the leading scientists involved in the research and development of Retatrutide. In no way is this doctor/scientist endorsing or advocating the purchase, sale, or use of this product for any reason. There is no affiliation or relationship, implied or otherwise, between Peptide Sciences and this doctor. The purpose of citing the doctor is to acknowledge, recognize, and credit the exhaustive research and development efforts conducted by the scientists studying this peptide. Dr. William C. Roell is listed in [1] and [2] under the referenced citations.
William C. Roell, PhD. received his bachelor’s degree in microbiology and biochemistry from Miami University. He obtained his doctorate in Cellular and Integrative Physiology from Indiana University School of Medicine doing work in cellular therapy and studying metabolic changes associated with adipocyte maturation. Joining Lilly in 2000, William worked with multiple drug discovery groups providing innovative approaches to translate therapeutic concepts from bench to bedside. More recently, he has supported efforts in diabetes biomarker discovery and target identification/advancement, impacting discovery and development efforts across Lilly’s Diabetes and Complications portfolio. William and his lab currently are active in drug discovery with a focus on diabetes and obesity. He has a particular interest in mechanisms by which incretin receptor modulation contributes to the profound benefits observed clinically with existing and emerging therapeutics.
Dr. William C. Roell is being referenced as one of the leading scientists involved in the research and development of Retatrutide. In no way is this doctor/scientist endorsing or advocating the purchase, sale, or use of this product for any reason. There is no affiliation or relationship, implied or otherwise, between Peptide Sciences and this doctor. The purpose of citing the doctor is to acknowledge, recognize, and credit the exhaustive research and development efforts conducted by the scientists studying this peptide. Dr. William C. Roell is listed in [1] and [2] under the referenced citations.
William C. Roell, PhD. received his bachelor’s degree in microbiology and biochemistry from Miami University. He obtained his doctorate in Cellular and Integrative Physiology from Indiana University School of Medicine doing work in cellular therapy and studying metabolic changes associated with adipocyte maturation. Joining Lilly in 2000, William worked with multiple drug discovery groups providing innovative approaches to translate therapeutic concepts from bench to bedside. More recently, he has supported efforts in diabetes biomarker discovery and target identification/advancement, impacting discovery and development efforts across Lilly’s Diabetes and Complications portfolio. William and his lab currently are active in drug discovery with a focus on diabetes and obesity. He has a particular interest in mechanisms by which incretin receptor modulation contributes to the profound benefits observed clinically with existing and emerging therapeutics.
Dr. William C. Roell is being referenced as one of the leading scientists involved in the research and development of Retatrutide. In no way is this doctor/scientist endorsing or advocating the purchase, sale, or use of this product for any reason. There is no affiliation or relationship, implied or otherwise, between Peptide Sciences and this doctor. The purpose of citing the doctor is to acknowledge, recognize, and credit the exhaustive research and development efforts conducted by the scientists studying this peptide. Dr. William C. Roell is listed in [1] and [2] under the referenced citations.
STORAGE INSTRUCTIONS:
All of Our Products are manufactured using the Lyophilization (Freeze Drying) process, which ensures that our products remain 100% stable for shipping for up to 24-36 month.
Once the peptides are reconstituted (mixed with bacteriostatic water), they just be stored in the fridge to maintain stability After reconstitution, the peptides will remain stable for up to 30 days.
Lyophilization is a unique dehydration process, also known as cryodesiccation, where the peptides are frozen and then subjected to low pressure. This causes the water in the peptide vial to sublimate directly from solid to gas, leaving behind a stable, crystalline white structure known as lyophilized peptide The puffy white powder can be stored at room temperature until you’re ready to reconstitute it with bacteriostatic water.
Once peptides have been received, it is imperative that they are kept cold and away from light. If the peptides will be used immediately, or in the next several days, weeks or months short-term refrigeration under 4c (39F) is generally acceptable. Lyophilized peptides are usually stable at room temperatures for several weeks or more, so if they will be utilized within weeks or months such storage is typically adequate.
However, for longer term storage (several months to years) it is more preferable to store peptides in a freezer at -80C (-112F).
When storin peptides for months or even years, freezing is optimal in order to preserve the peptide’s stability.
Dermorphin
10mg
Insulin
Long Lasting 3mg
Fast Acting 3mg
Somatropin HGH
10iu
15iu
AOD 9604
2mg
5mg
ВРС 157
2mg
5mg
10mg
NAD+
100mg
500mg
1000mg
Retatruitide
5mg
10mg
15mg
20mg
Tirz
5mg
10mg
20mg
30mg
40mg
50mg
60mg
Viagra
100mg (30 Pills)
Mots C
10mg
Cagri
10mg
Lipo C
10mg
Kisspeptin-10
5mg
Semax
10mg
Collagen Peptide Powder
9.330z
RETA Overview
Reta is a new entrant into the rapidly-expanding space of anti-obesity peptides. It is known as a GGG tri-agonist. This means that retatrutide works at all of the incretin receptors including GLP-1 and GIP as well as the glucagon receptor itself. Research indicates that retatrutide may be the most effective weight loss peptide yet developed, with some studies showing a rapid and sustained weight loss response as high as 24% of total body weight[1]. Reta is thought to promote weight loss by increasing energy expenditure as well as decreasing energy consumption. It does the former via action at the glucagon receptor and the latter through both central and peripheral appetite control.
RETA Structure
Sequence: YA1QGTFTSDYSIL2LDKK4AQA1AFIEYLLEGGPSSGAPPPS3
Molecular Formula: C223H343F3N46O70
Molecular Weight: 4731.33 g/mol
PubChem SID: 474492335
CAS Number: 2381089-83-2
Synonyms: LY-3437943, NOP2Y096GV
RETA Research
What is Reta?
Reta, as mentioned, is a GGG tri-agonist. Reta is a fatty acid acylated single peptide that combines GCGR, GIPR, and GLP-1R activities. It is based off of the GIP peptide backbone that is heavily modified. Modification of this backbone has allowed retatrutide to bind to albumin in the bloodstream. This, in turn, means that the drug remains in the blood for a prolonged period of time. This extended half-life means that retatrutide only needs to be taken once per week[2]. It wide spectrum of activity allows retatrutide to bind to several difference incretin receptors and produce specific effects as follows.
Gastric Inhibitor Peptide Receptor (GIPR): Also called the glucose-dependent insulinotropic polypeptide receptor, this receptor is found in the central nervous system as well as throughout the GI tract and body. It appears to play important roles in the central mechanisms that affect hunger and is thought to play a role in sending “fullness” signals from the GI tract to the brain.
Glucagon-like Peptide Receptor-1 (GLP-1R): Activation of this receptor leads to slowing of gastric emptying. Slowed gastric emptying sends signals to the brain to decrease food intake and can therefore help to control energy consumption. Peptides targeting this receptor were originally developed to treat type 2 diabetes, but have since been found to improve weight loss and decrease the risk of certain forms of heart disease. They are under investigation for the treatment of depression, reward system disorders (e.g., alcoholism, addiction), polycystic ovarian syndrome, and non-alcoholic fatty liver disease.
Glucagon Receptor (GCGR): The glucagon receptor is found mainly in the liver and kidney. Mutations in this receptor are associated with certain forms of type 2 diabetes. By binding to this receptor, reta increases glucagon production, which stimulates the breakdown of stored forms of energy like fat and glycogen. This leads to an increase in basal metabolism (even during sleep) that increases weight loss in general and fat loss specifically.
How Does Reta Work?
In vivo research, in humans, indicates that retatrutide activates and is a full agonist of all of the incretin receptors including GIPR, GLP-1R, and GCGR. Reta was specifically designed to be highly potent at the GIPR and GLP-1R locations. As a result, reta is one of the most potent incretins available and thus has strong effects on both gastric emptying and the central control of hunger/satiety. Research shows that the bulk of reta’s effects are driven by loss of fat mass that is probably the result of a larger and more prolonged reduction in food intake compared to similar peptides. Decreased food intake, especially as occurs early in the use of the peptide, jump starts fat oxidation. This sets the stage for prolonged weight loss by altering basal metabolism and overcoming the hormonal forces that perpetuate obesity[2].
The bulk of reta’s benefit is a result of its ability to decrease energy intake via delayed gastric emptying and increased control of hunger signals in the central nervous system. That said, the ability of the peptide to increase energy expenditure is also statistically significant and should not be discounted.
GIPR Effect: (glucose-dependent insulinotropic polypeptide receptor)
Agonism of the GIPR leads to decreased gastric acid secretion and gastrin release. Gastrin is a peptide hormone that stimulates the release hydrochloric acid and histamine in the stomach. These effects help to slow digestion and reduce transit through the GI tract. As a result, action on the GIPR can lead to increased feelings of fullness.
GLP-1R Effects: (glucagon-like peptide-1 receptor)
Agonism of the GLP-1R is well known to delay gastric emptying. Research in both rodents and humans supports this. Gastric emptying (GE) is an important determinant of the glycemic response following food intake. Research indicates that slowing GE can reduce food intake and thus impact weight loss.
Research in mice reveals that GLP-1R is the only receptor of the three to affect GE, and thus the delay of GE caused by reta is no greater than the delay caused by sema, tirz, lira, or any of the other GLP-1R agonists. Interestingly, however, is the difference in dose to achieve full effect on GE. Research shows that reta has the same efficacy as semaglutide at a dose that is more than 30 times smaller[3]. As with sema, however, the effects of reta on GE wane over time. This decrease in effect of a therapeutic over time is referred to as tachyphylaxis and may, in some cases, necessitate a drug holiday to help restore effects.
GCGR Effects: (G-protein-coupled receptor)
It wasn’t fully understood until relatively recently that glucagon plays an important role in regulating hunger and energy expenditure. Research now reveals that glucagon signals the brain from the gut via the vagal nerve. This signaling promotes feelings of fullness and is regulated by glucagon concentrations in the portal circulation of the liver. In mouse models, the administration of glucagon has resulted in a 20% weight loss[4].
Additional research has shown that glucagon can increase energy expenditure. This effect has been observed in both animal and human trials. This particular effect is not mediated through the GCGR, but rather through via FGF21. FGF21 is a protein secrete by the liver that regulated sugar intake and preferences for sweet foods, among a host of other functions. Mutations in this protein have been identified in those with a “sweet tooth” [5]. FGF21 regulates the uptake of glucose by adipocytes (fat cells). Treatment of animals with FGF21 results in increased energy expenditure, fat utilization and lipid excretion. Studies in mice show that activation of FGF21 can lead to a 20% weight reduction primarily via increased fat loss[6]. This occurs without a change in total calorie intake, indicating a change in metabolic rate. Mice given an FGF21 infusion have demonstrated higher energy expenditure both during wakefulness and during sleep. This is likely mediated through effects on mitochondrial activity.
How Effective is Reta for Weight Loss?
Research indicates that retatrutide is likely the most effect incretin-based peptide for weight loss yet developed. In a study in rodents, for instance, just 10 days of reta treatment leads to decreases in total body weight greater than those seen with sema. This occurs when the peptides are administered at the same doses. If reta is given at a lower dose that sema, then it produces similar weight loss effects but with decreased risk of side effects[3]. Thus, retatrutide may offer an alternative treatment option for those who are somewhat intolerant of the side effects of sema.
A phase 2 study in humans has showed that reta can produced significant reductions in body weight. In fact, trial participants given the highest dose of the peptide lose approximately 20 pounds in just 12 weeks[1]. In another trial, individuals treated for 26 weeks showed changes in waist circumference ranging from -2.1 cm to -10.2 cm[7]. In other words, people taking reta in this trial lost anywhere from 1 inch to ~5 inches off of their waist in just 6 months. Finally, in a trial published in the New England Journal of Medicine, weight loss from reta varied in a dose-dependent manner over the 48 weeks of the trial. Individuals given the lowest dose of the peptide lost 8.7% of their total body weight while those given the highest dose lost more than 24% of their total body weight[8]. Similar results were published in a JAMA article as well[9].
Reta and Diabetes Research
In phase 2 trials, retatrutide has produced significant reductions in glycated hemoglobin (hemoglobin A1c) levels[10]. Hemoglobin is the compound in blood that carries oxygen. Glycated hemoglobin is hemoglobin that has been chemically linked to a sugar. High levels of glycated hemoglobin are caused by chronically high levels of blood sugar and are associated with diabetes. In fact, HBA1c levels can be used to monitor long-term blood sugar control in those suffering from diabetes. Keeping these levels lower is critical not only to good blood sugar control, but to preventing the long-term effects of diabetes including cardiovascular disease, nerve damage, kidney injury, and eye problems.
Reta and Heart Health Research
It has long been known that infusing elevated doses of glucagon into those with heart failure can augment heart rate and cardiac contractility. Pharmacological administration of glucagon, typically in milligram quantities, is commonly employed in addressing acute cardiac depression resulting from overdoses of calcium channel antagonists or beta-blockers, despite limited research in this area. Interestingly, glucagon concentrations within the normal physiological range seem to have no discernible impact on heart rate or contractility[11].
The impact of reta on heart health has not been directly assessed in humans, but it has been assessed in cynomolgus monkeys. In the past, it was thought that elevated actions of glucagon were associated with diabetes. That is to say, scientists thought that lower glucagon would lead to improved outcomes in diabetes. Thus, monoclonal glucagon antibodies, glucagon receptor antagonists (peptide and non-peptide) and molecules targeting the expression of GCGR have all been tested as potential treatments. Research on these agents, however, revealed a number of major obstacles including limited efficacy, the risk of iatrogenic hypoglycemia, and other safety issues related to lack of specificity of glucagon blockade, immunogenicity and toxicity. This really should not have come as any surprise as the rise in glucagon levels in diabetes is likely a consequence of the disease and not a cause of it.
Research also indicates that incretins have beneficial effects on the cardiovascular system by decreasing blood pressure, improving left ventricular function, endothelium-dependent vasodilation, and by increasing endothelial progenitor cells. In other words, glucagon and related molecules appear to improve heart health[12]. Supporting this notion is the fact that a number of incretin agonists (e.g. sema, lira) have been associated with improvements in cardiovascular outcomes in diabetes. As a result, these peptides are now under investigation for direct use in heart disease. Reta is likely to show improved results given its more extensive effects on glucagon levels, but the exact effects will have to await more detailed clinical and benchtop trials. These findings indicate that retatrutide and similar molecules may be beneficial to regeneration in the cardiovascular as well as helping to prevent cardiovascular disease in the first place.
As mentioned, a limited, non-clinical cardiovascular study of reta in monkeys has been undertaken. This study revealed higher heart rates at all dose levels with a dose dependent effect overall. At the same time reta was increasing heart rate, it was decreasing blood pressure in the monkeys. Unfortunately, this study was limited in both duration and number of individuals under investigation. Thus, while it can offer some foundation on which to ground speculation, it cannot provide any definitive information about reta and its long-term effects on cardiovascular health.
Reta Summary
Reta is an incretin mimetic and GGG agonist. It binds to glucagon receptors, gastric inhibitory peptide receptors, and glucagon-like peptide-1 receptors. This triple activity has been associated with significant weight loss (24% of body weight at 6 months) in clinical trials. This outcome makes reta the most effective of incretin peptides to date and thus it is under intense investigation as a weight loss agent. There is some hope that reta may also have beneficial cardiovascular effects and might therefore be useful in the treatment of heart disease complicated by diabetes as well as heart disease in general.
About the Author
The above literature was researched, edited and organized by Dr. Logan, M.D. Dr. Logan holds a doctorate degree from Case Western Reserve University School of Medicine and a B.S. in molecular biology.
Scientific Journal Author
William C. Roell, PhD. received his bachelor’s degree in microbiology and biochemistry from Miami University. He obtained his doctorate in Cellular and Integrative Physiology from Indiana University School of Medicine doing work in cellular therapy and studying metabolic changes associated with adipocyte maturation. Joining Lilly in 2000, William worked with multiple drug discovery groups providing innovative approaches to translate therapeutic concepts from bench to bedside. More recently, he has supported efforts in diabetes biomarker discovery and target identification/advancement, impacting discovery and development efforts across Lilly’s Diabetes and Complications portfolio. William and his lab currently are active in drug discovery with a focus on diabetes and obesity. He has a particular interest in mechanisms by which incretin receptor modulation contributes to the profound benefits observed clinically with existing and emerging therapeutics.
Dr. William C. Roell is being referenced as one of the leading scientists involved in the research and development of Retatrutide. In no way is this doctor/scientist endorsing or advocating the purchase, sale, or use of this product for any reason. There is no affiliation or relationship, implied or otherwise, between Peptide Sciences and this doctor. The purpose of citing the doctor is to acknowledge, recognize, and credit the exhaustive research and development efforts conducted by the scientists studying this peptide. Dr. William C. Roell is listed in [1] and [2] under the referenced citations.
Reference Citations
William C. Roell, PhD. received his bachelor’s degree in microbiology and biochemistry from Miami University. He obtained his doctorate in Cellular and Integrative Physiology from Indiana University School of Medicine doing work in cellular therapy and studying metabolic changes associated with adipocyte maturation. Joining Lilly in 2000, William worked with multiple drug discovery groups providing innovative approaches to translate therapeutic concepts from bench to bedside. More recently, he has supported efforts in diabetes biomarker discovery and target identification/advancement, impacting discovery and development efforts across Lilly’s Diabetes and Complications portfolio. William and his lab currently are active in drug discovery with a focus on diabetes and obesity. He has a particular interest in mechanisms by which incretin receptor modulation contributes to the profound benefits observed clinically with existing and emerging therapeutics.
Dr. William C. Roell is being referenced as one of the leading scientists involved in the research and development of Retatrutide. In no way is this doctor/scientist endorsing or advocating the purchase, sale, or use of this product for any reason. There is no affiliation or relationship, implied or otherwise, between Peptide Sciences and this doctor. The purpose of citing the doctor is to acknowledge, recognize, and credit the exhaustive research and development efforts conducted by the scientists studying this peptide. Dr. William C. Roell is listed in [1] and [2] under the referenced citations.
William C. Roell, PhD. received his bachelor’s degree in microbiology and biochemistry from Miami University. He obtained his doctorate in Cellular and Integrative Physiology from Indiana University School of Medicine doing work in cellular therapy and studying metabolic changes associated with adipocyte maturation. Joining Lilly in 2000, William worked with multiple drug discovery groups providing innovative approaches to translate therapeutic concepts from bench to bedside. More recently, he has supported efforts in diabetes biomarker discovery and target identification/advancement, impacting discovery and development efforts across Lilly’s Diabetes and Complications portfolio. William and his lab currently are active in drug discovery with a focus on diabetes and obesity. He has a particular interest in mechanisms by which incretin receptor modulation contributes to the profound benefits observed clinically with existing and emerging therapeutics.
Dr. William C. Roell is being referenced as one of the leading scientists involved in the research and development of Retatrutide. In no way is this doctor/scientist endorsing or advocating the purchase, sale, or use of this product for any reason. There is no affiliation or relationship, implied or otherwise, between Peptide Sciences and this doctor. The purpose of citing the doctor is to acknowledge, recognize, and credit the exhaustive research and development efforts conducted by the scientists studying this peptide. Dr. William C. Roell is listed in [1] and [2] under the referenced citations.
William C. Roell, PhD. received his bachelor’s degree in microbiology and biochemistry from Miami University. He obtained his doctorate in Cellular and Integrative Physiology from Indiana University School of Medicine doing work in cellular therapy and studying metabolic changes associated with adipocyte maturation. Joining Lilly in 2000, William worked with multiple drug discovery groups providing innovative approaches to translate therapeutic concepts from bench to bedside. More recently, he has supported efforts in diabetes biomarker discovery and target identification/advancement, impacting discovery and development efforts across Lilly’s Diabetes and Complications portfolio. William and his lab currently are active in drug discovery with a focus on diabetes and obesity. He has a particular interest in mechanisms by which incretin receptor modulation contributes to the profound benefits observed clinically with existing and emerging therapeutics.
Dr. William C. Roell is being referenced as one of the leading scientists involved in the research and development of Retatrutide. In no way is this doctor/scientist endorsing or advocating the purchase, sale, or use of this product for any reason. There is no affiliation or relationship, implied or otherwise, between Peptide Sciences and this doctor. The purpose of citing the doctor is to acknowledge, recognize, and credit the exhaustive research and development efforts conducted by the scientists studying this peptide. Dr. William C. Roell is listed in [1] and [2] under the referenced citations.
STORAGE INSTRUCTIONS:
All of Our Products are manufactured using the Lyophilization (Freeze Drying) process, which ensures that our products remain 100% stable for shipping for up to 24-36 month.
Once the peptides are reconstituted (mixed with bacteriostatic water), they just be stored in the fridge to maintain stability After reconstitution, the peptides will remain stable for up to 30 days.
Lyophilization is a unique dehydration process, also known as cryodesiccation, where the peptides are frozen and then subjected to low pressure. This causes the water in the peptide vial to sublimate directly from solid to gas, leaving behind a stable, crystalline white structure known as lyophilized peptide The puffy white powder can be stored at room temperature until you’re ready to reconstitute it with bacteriostatic water.
Once peptides have been received, it is imperative that they are kept cold and away from light. If the peptides will be used immediately, or in the next several days, weeks or months short-term refrigeration under 4c (39F) is generally acceptable. Lyophilized peptides are usually stable at room temperatures for several weeks or more, so if they will be utilized within weeks or months such storage is typically adequate.
However, for longer term storage (several months to years) it is more preferable to store peptides in a freezer at -80C (-112F).
When storin peptides for months or even years, freezing is optimal in order to preserve the peptide’s stability.
